TV in Pharma Marketing: Why Omnichannel Strategies Break Without It
Sarah Moss
February 4, 2026
11
minutes read
Pharma TV marketing is evolving fast as privacy limits tighten and digital-first approaches stall. In this article, we’ll explain how TV can anchor omnichannel efforts and still be measured credibly.
If you run U.S. pharma marketing, you already know the paradox: you’re expected to prove business outcomes while operating inside some of the strictest privacy and regulatory boundaries in advertising. Meanwhile, your audience spans wildly different viewing behaviors—patients, caregivers, and HCPs do not move through the journey in one neat funnel.
Here’s the bet we’re making: TV is the closest thing pharma has to a “shared layer” across the journey. Not because it’s magical, but because it still delivers reach at scale, it’s increasingly addressable through streaming, and it can be measured in privacy-safe ways that align with how pharma outcomes are defined (scripts, new-to-brand starts, adherence, and follow-up actions).
⚡ Omnichannel isn’t more channels. It’s one system that behaves predictably.
From there, we can rebuild omnichannel around TV as the backbone—then connect digital, search, and point-of-care into a plan that behaves like a single operating model.
The reality of pharma omnichannel in 2026
Omnichannel in pharma is often described as orchestrated, personalized, and consistent. The reality is more constrained—and more interesting.
The U.S. market is structurally different
The United States is one of the only countries that permits direct-to-consumer (DTC) prescription drug advertising at scale, alongside New Zealand. That single fact changes the media math, because awareness and education aren’t optional add-ons; they’re a core growth lever.
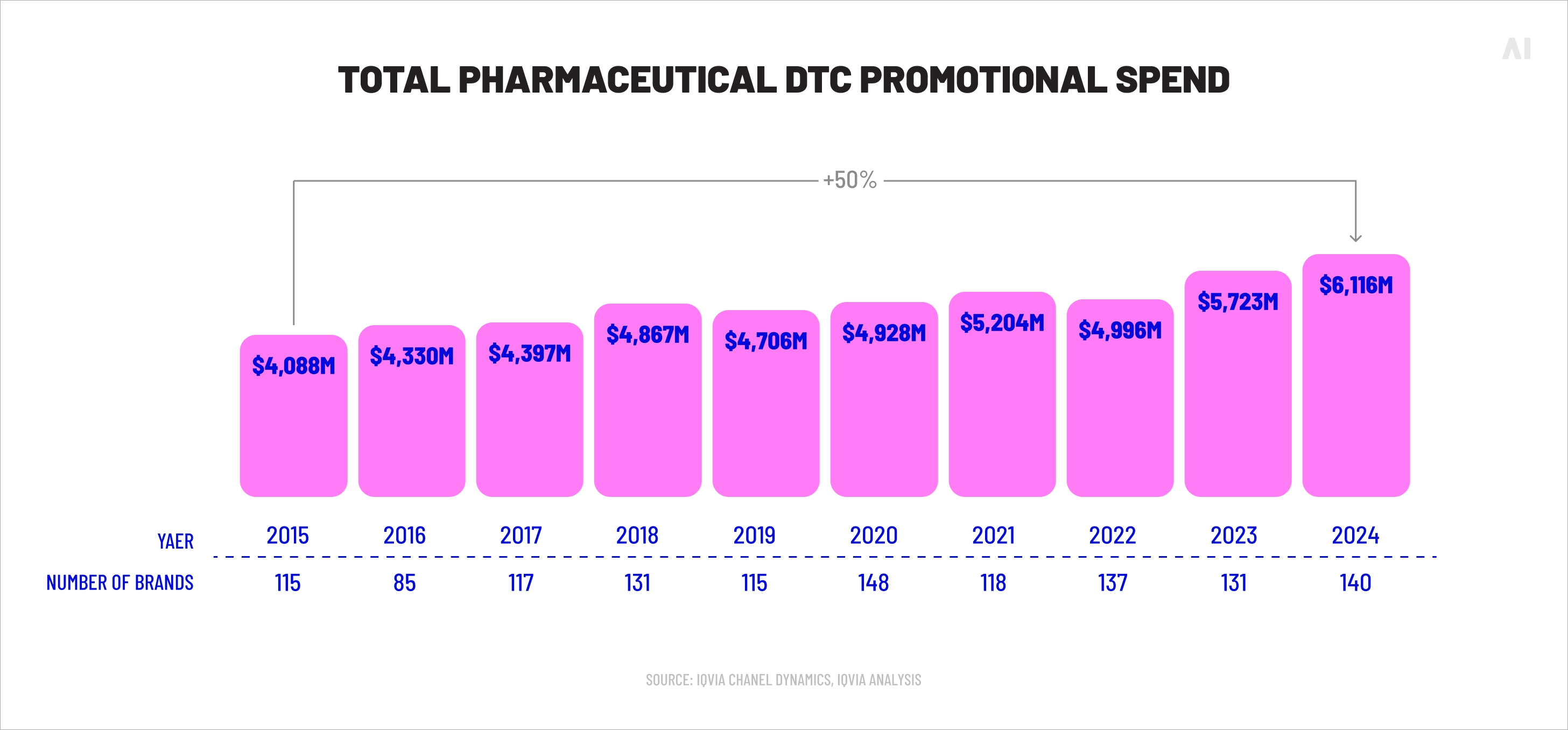
Total pharmaceutical DTC promotional spend (Source)
The money shows where pressure is
Healthcare and pharma advertising is large and still expanding. EMARKETER estimated~$30B in U.S. healthcare + pharma ad spending in 2024, with digital continuing to take share. By late 2025, EMARKETER reportedpharma TV ad spending reached ~$5.4B through November 2025 (surpassing 2024’s full-year ~$5.1B), based on iSpot data.
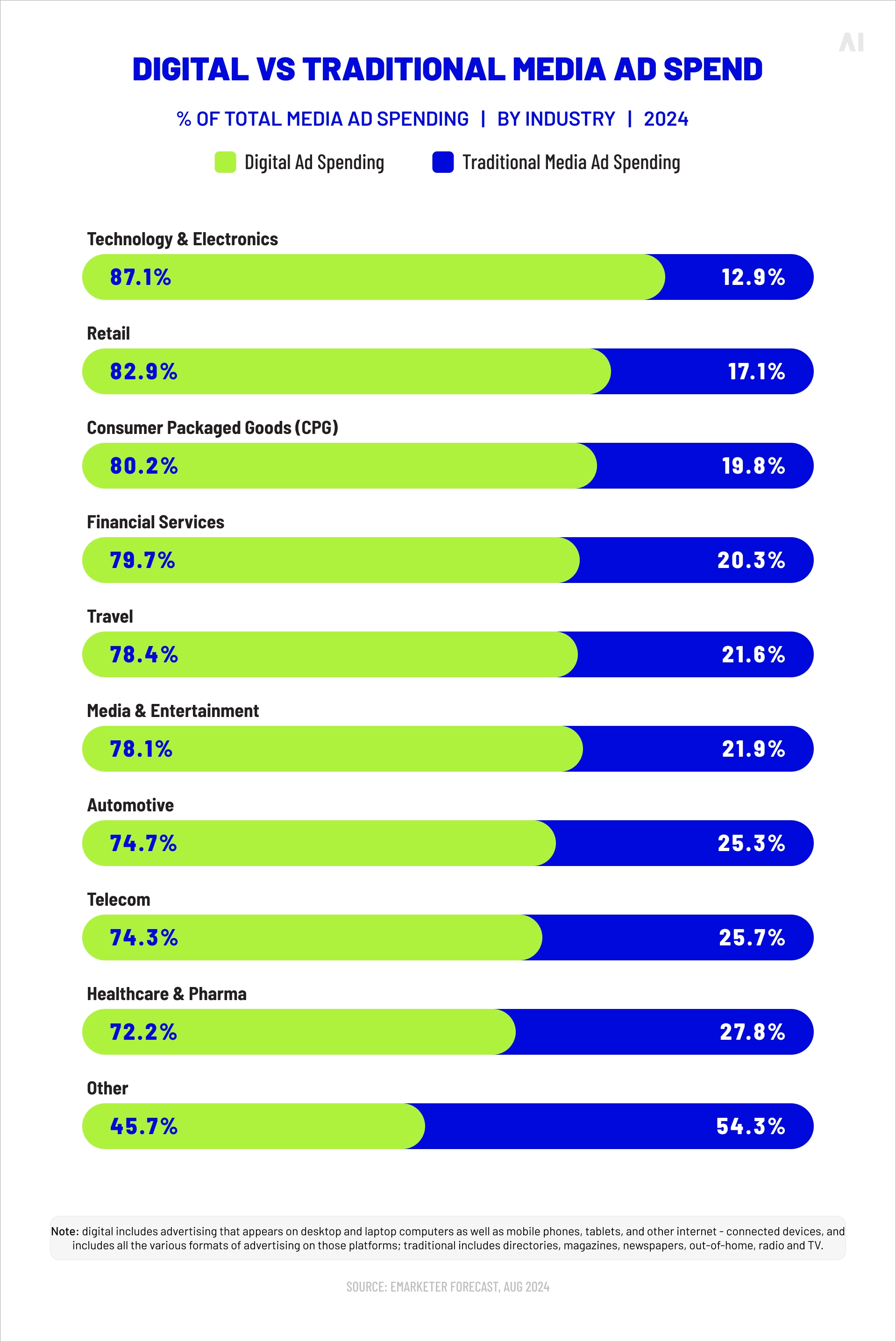
Digital vs traditional media ad spend by industry (Source)
Those numbers matter for one reason: TV is not behaving like a legacy channel in pharma budgets. It’s still a primary investment, even as teams talk “digital-first.”
Audience behavior has shifted, but not away from TV
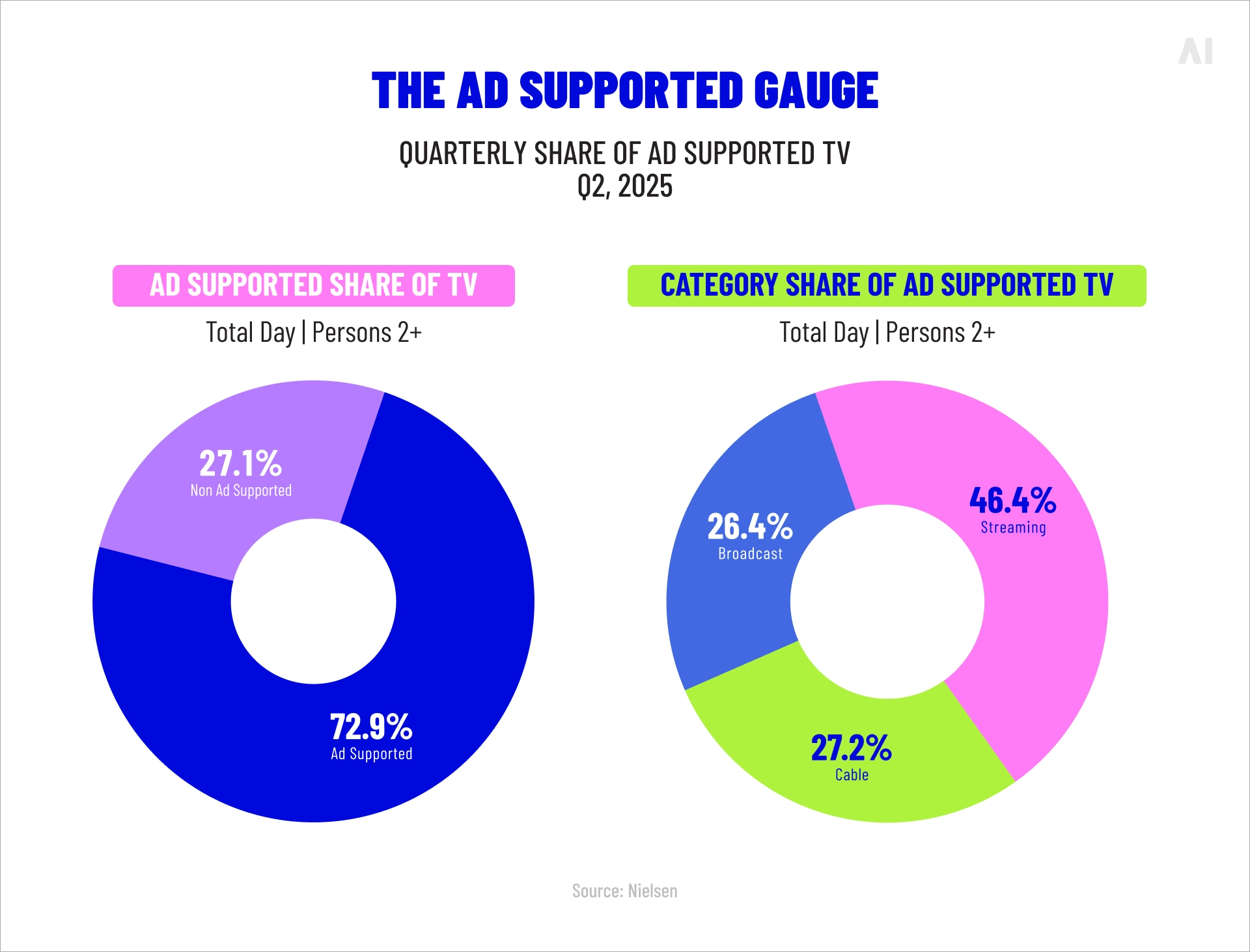
Nielsen’s Gauge showed streaming hit 44.8% of total TV usage in May 2025, edging past broadcast + cable combined for the first time.Then Nielsen’s Ad Supported Gauge found ad-supported viewing accounted for 72.9% of overall TV viewing in Q3 2025, with streaming representing a large chunk of ad-supported time.
Translation: “TV” is now a blended environment—linear still delivers scale, while streaming delivers incremental reach, household-level delivery, and new measurement surfaces.
Regulation and scrutiny are rising (and that changes creative and proof)
In September 2025, HHS and FDA announced actions and messaging focused on prescription drug ad transparency and enforcement, with FDA also publicizing a crackdown on deceptive drug advertising. Whether or not any specific policy direction sticks long-term, the implication is immediate: pharma marketers need better proof, tighter substantiation, and cleaner measurement.
Key takeaways (reality check):
TV still anchors DTC scale in the U.S., even as budgets shift across formats.
Streaming has become mainstream TV behavior, not a niche.
Regulatory scrutiny raises the bar on proof, which pushes measurement maturity from “nice-to-have” to survival.
That reality sets up the next question: if digital keeps growing, why do so many digital-first pharma strategies stall?
{{26-TV-in-Pharma-Marketing-1="/tables"}}
💡 For a primer on trends shaping up in 2026, see the dedicated report: 2026 media trends.
Why digital-first strategies hit a ceiling in pharma
Digital-first works—until it doesn’t. In pharma, the ceiling tends to show up in three places: privacy, saturation, and missing the “shared layer” of the journey.
Privacy rules don’t just restrict targeting
Pharma can’t treat health data like retail data, and it can’t behave like a typical performance advertiser without triggering compliance and consumer trust issues. AdExchanger summarized the core tension well: pharma struggles with targeting and measurement because patient data is highly regulated, and condition-based targeting can feel invasive.
At the broader advertising level, signal loss and privacy legislation continue to tighten the learning loop. IAB’s State of Data 2024reported that 95% of data decision-makers expected continued legislation and signal loss, and 3 in 4 expected reduced ability to collect integral consumer data.
% relying on legal support due to signal loss (Source)
Digital-first plans often assume they can “optimize their way out” of weak performance. In pharma, you frequently cannot observe enough to optimize safely.
Digital can saturate before it scales the full journey
Search and social are powerful for capturing existing intent. But pharma demand creation still relies heavily on education, awareness, and memory—especially for chronic conditions and categories where patients aren’t actively shopping.
EMARKETER noted that pharma’s digital spend skews toward paid search, and also pointed to how difficult it is to drive “offline” outcomes like prescriptions from digital interactions alone. When digital is optimized primarily for clicks, it can miss the mid-funnel work that creates future intent.
The pharma journey requires shared context (and digital often fragments it)
The patient journey isn’t one device, one platform, or one decision-maker.
Patients see an ad, then talk to a physician.
Caregivers influence the next step.
HCPs have their own evidence needs and time constraints.
Formularies, prior auth, and affordability shape what happens next.
A digital-first plan can end up as a set of platform-specific tactics with no consistent narrative thread. TV, for all its imperfections, is often the only channel that delivers shared context at population scale.
⚡ Digital can be precise. TV can be shared. Pharma needs both.
So if digital-first hits a ceiling, what does TV actually do across the journey—beyond “awareness”?
TV works in pharma because it can do three jobs at once:
create broad awareness and memory,
support education and reassurance,
connect to measurable outcomes through modern identity and clean-room approaches (when set up correctly).
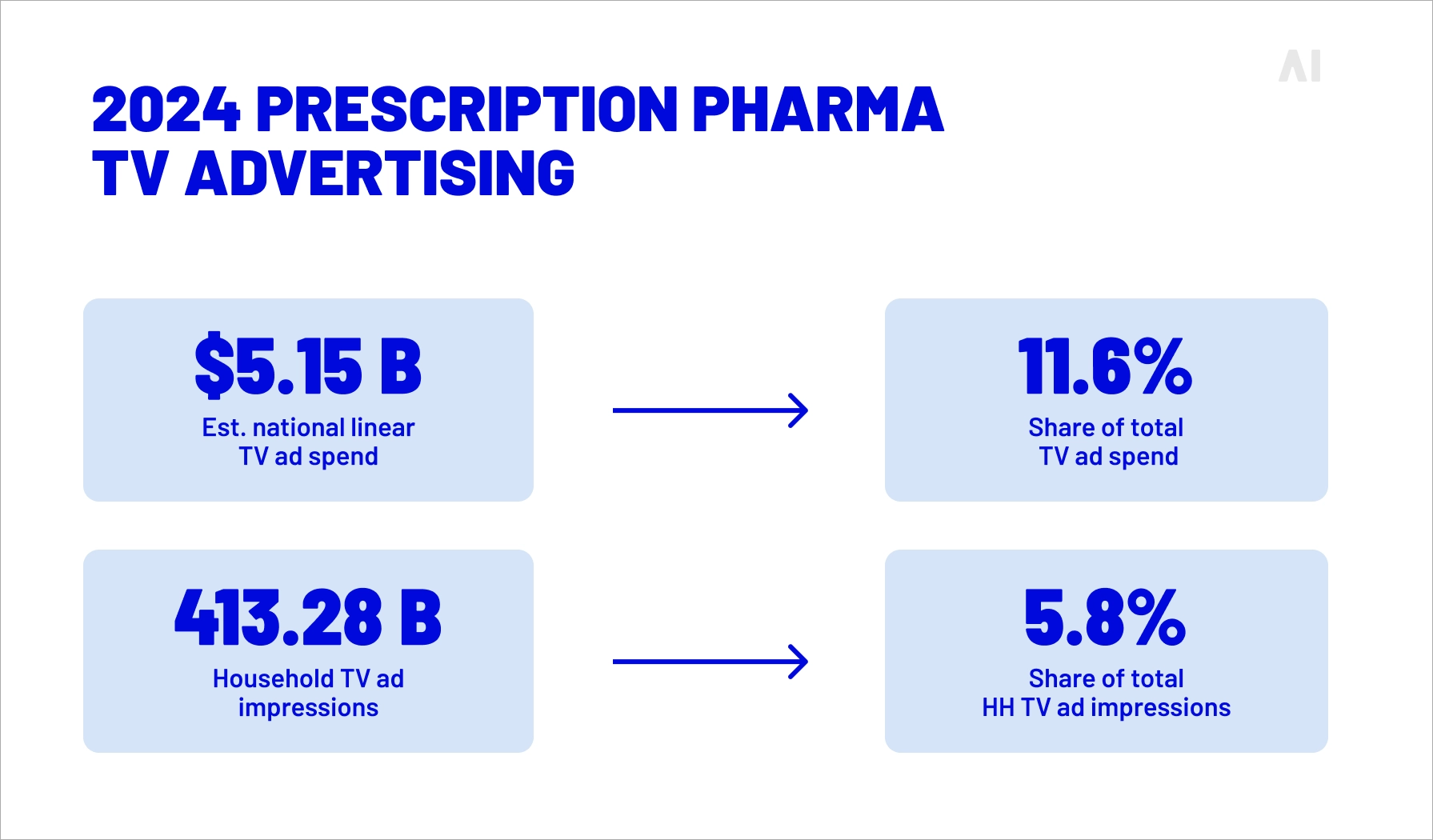
iSpot’s 2024 transparency report puts hard numbers on the baseline: prescription pharma advertisers invested over $5.15B in linear TV ads in 2024, delivering 413B impressions across 271 brands. This is not a channel pharma is “moving on” from. It’s a channel pharma is re-instrumenting.
2024 prescription pharma TV advertising in numbers (Source)
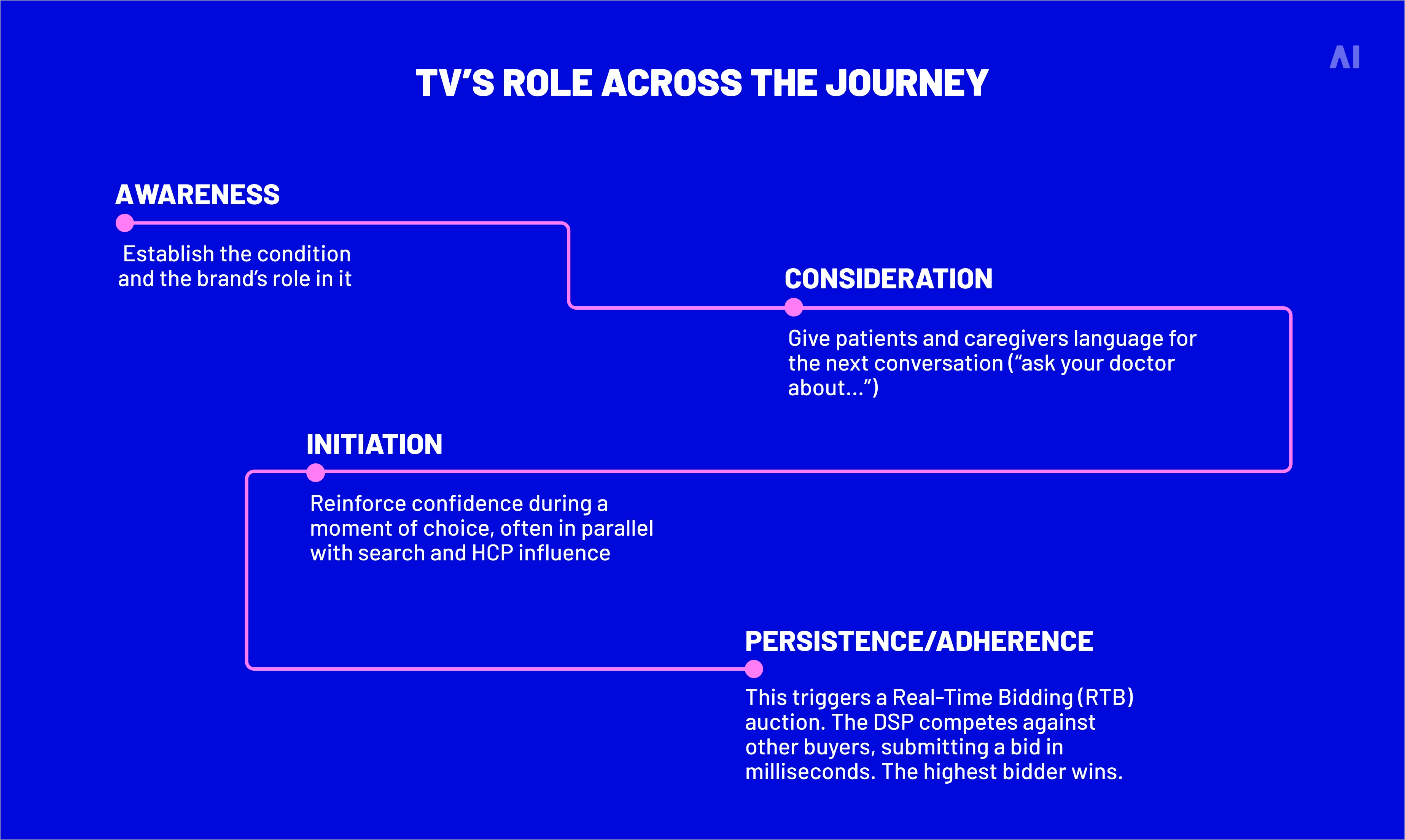
Before we break out linear, CTV, and addressable, it helps to map where TV contributes across the journey.
⚡ Almost everyone has seen prescription drug ads, which is exactly why TV remains a behavior-shaping channel in the U.S. The point is not that TV reaches “everyone”; it’s that TV creates shared awareness faster than most digital-first plans can.
Linear TV and pharma marketing
Linear is still the fastest path to broad, repeated exposure in a regulated category. It also gives pharma a familiar set of buying patterns (dayparts, networks, tentpole programming) and an environment that tends to be perceived as more “mainstream” than many digital placements.
iSpot also noted a concentration dynamic: over 52% of national TV pharma spend went into just five networks in 2024. That implies two things:
pharma still values premium context and predictable delivery, and
there’s likely meaningful waste unless cross-platform planning is designed to manage frequency.
Where linear shines:
Launch or relaunch moments where memory matters
Categories with high caregiver influence
Broad public education and condition framing
Where linear strains:
Frequency waste at the household level
Limited “next-step” interactivity
Harder to connect to outcomes without additional infrastructure
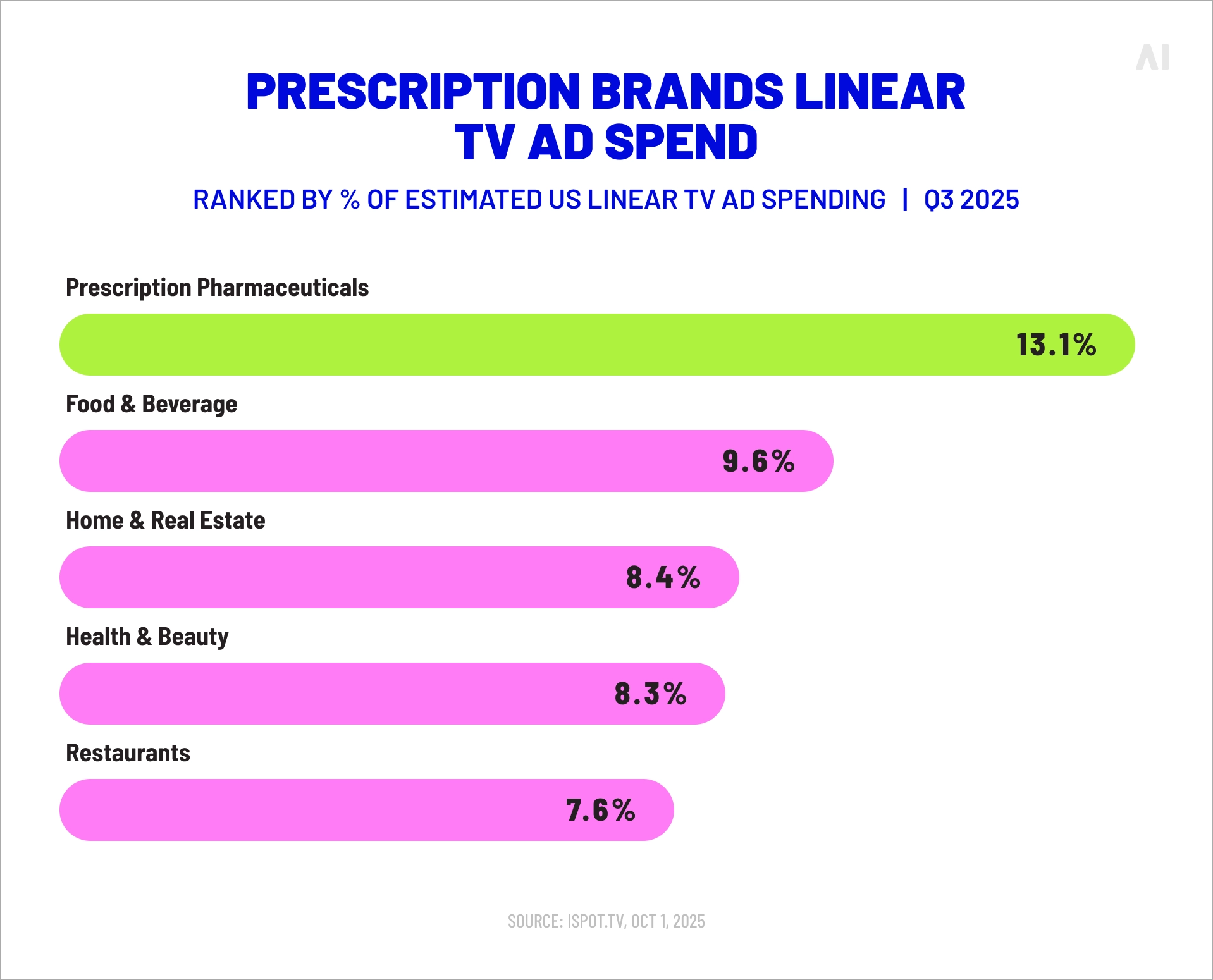
Prescription brands linear TV ad spend Q3 2025 (Source)
Connected TV and pharma TV marketing
CTV is not “digital video on a TV screen.” It behaves differently because it blends:
TV attention (lean-back viewing),
digital-like delivery mechanics (household-level ad serving),
and measurement pathways that can be privacy-safe (when you avoid individual-level health targeting).
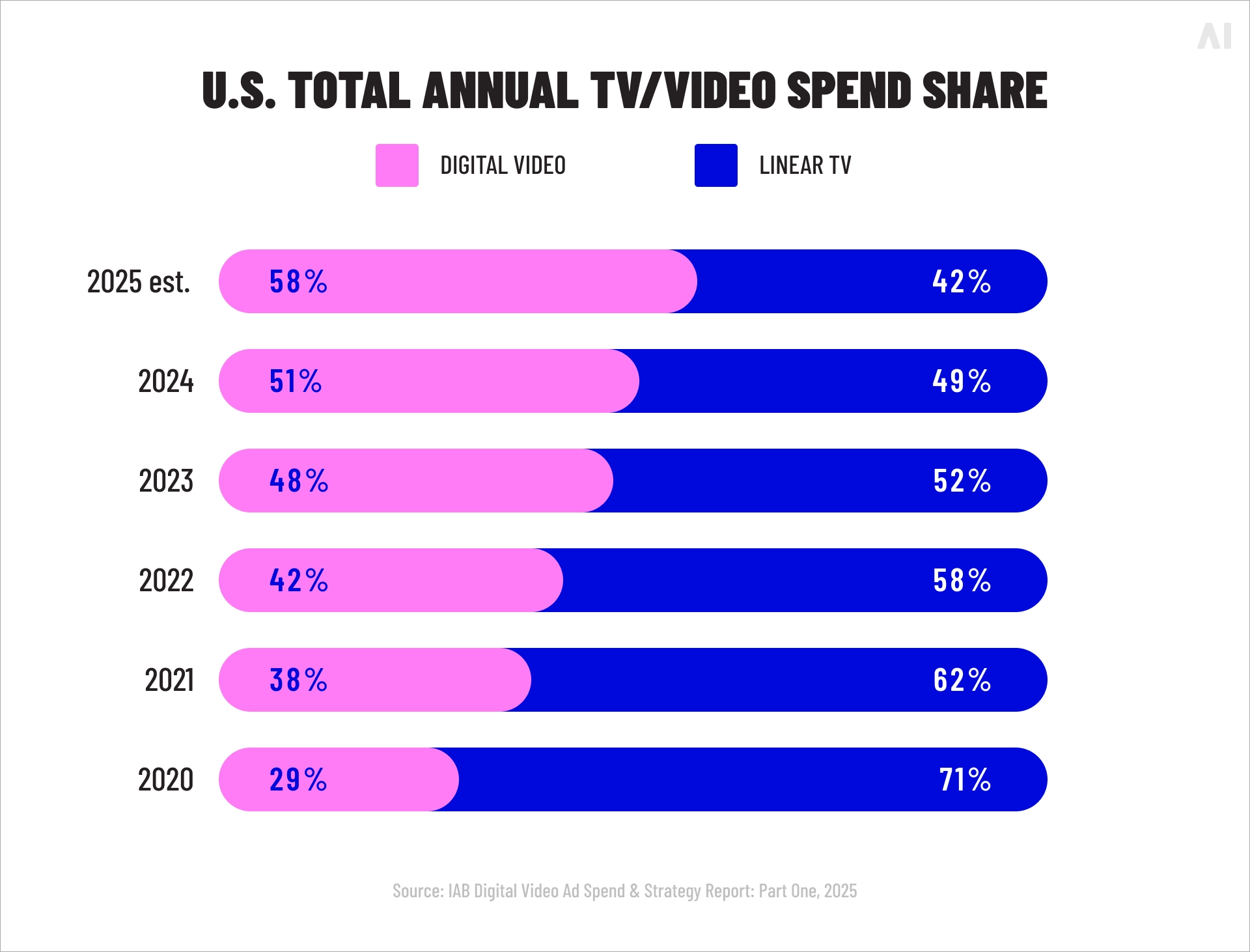
The macro trend is obvious: IAB reported digital video ad spend grew 18% in 2024 to $64B and was projected to reach $72B in 2025, with digital video expected to capture nearly 60% of total TV/video ad spend in 2025. Pharma doesn’t need to follow every macro trend—but these shifts expand inventory, tooling, and measurement options that pharma can use.
Aligning exposure with regional access realities (within compliant bounds)
A useful detail from iSpot: weight-loss brands like Zepbound used streaming first to test messaging before expanding to linear. That’s a modern pattern: treat streaming as a faster creative feedback loop, then scale what works.
Measuring TV in pharma is not about finding a perfect attribution model. It’s about building a stack of evidence that holds up under privacy constraints and reflects how pharma outcomes happen.
A practical measurement system usually includes four layers:
Delivery and audience truth (reach, frequency, incremental reach)
Clinical/commercial outcomes (new scripts, refills, adherence signals)
Incrementality (did TV drive outcomes that wouldn’t have happened?)
{{26-TV-in-Pharma-Marketing-3="/tables"}}
The privacy-first constraint (and the opportunity)
AdExchanger’s reporting on Blockgraph and Datavant describes the direction of travel: use clean room approaches to match de-identified claims data with anonymized TV exposure data to measure outcomes like script lift, without enabling household-level targeting based on claims.
⚡ If TV can drive real-world actions, you should expect to see it in outcomes like doctor conversations and prescription behavior, not just site traffic. In a KFF poll, a meaningful share of adults said they talked to a doctor about a medicine they saw advertised, and many reported receiving that prescription.
This matters because it aligns measurement with pharma’s real outcome language:
new-to-brand starts
switches
persistence and refills (where available)
follow-up actions that correlate with treatment initiation
What “good” looks like (a realistic checklist)
A TV measurement plan is usually stronger when it includes:
A defined outcome hierarchy: Not every campaign should be judged on scripts. Some should be judged on qualified actions that are known precursors.
A test design you can defend: Geo-based tests, holdouts, matched markets, or controlled comparisons that don’t require individual-level tracking.
A clean-room or privacy-safe match strategy: Especially if you want to connect exposure to claims-based outcomes.
A cross-channel view of frequency: Because overexposure can quietly kill efficiency.
A compliance-forward data policy: That treats health data and sensitive inference as a “do not touch” zone for targeting, while still enabling aggregated learning.
Don’t skip the “incrementality” conversation
If your organization is still relying on last-click style thinking, TV will look worse than it is, because TV does not behave like a click channel.
One reason this conversation is intensifying is the broader data environment: as noted earlier, IAB found widespread expectation of ongoing signal loss and reduced ability to collect consumer data.
TV measurement in pharma is evolving not because it’s trendy, but because it’s one of the few places where privacy-safe outcome linkage is becoming more standardized.
When TV becomes the backbone, three things change: planning, creative, and organizational behavior.
Planning becomes journey-based instead of channel-based
Instead of asking, “How much CTV should we buy?” you ask:
What does the audience need to believe at each stage?
What is the next best action we want to trigger?
Where do we need shared context vs personalized reinforcement?
This shift turns TV from a blunt instrument into a sequencing and reinforcement engine.
Creative becomes modular (without losing the big idea)
Pharma creative often has to carry a lot: condition framing, benefits, safety balance, support programs, and brand trust signals.
A TV-led system encourages:
a consistent “master narrative” (what this brand stands for in the category),
plus modular variants (by audience proxy, region, or stage),
plus digital companions that handle depth and FAQs.
iSpot’s 2024 report highlights how brands are evolving creative and cross-platform strategy, including examples of streaming-led testing before scaling.
{{26-TV-in-Pharma-Marketing-4="/tables"}}
Measurement becomes an organizational forcing function
Here’s the underappreciated advantage: once you set up TV measurement that connects to outcomes, teams stop arguing about platform vanity metrics and start aligning on the same scorecard.
The above-mentioned Blockgraph–Datavant approach described by AdExchanger is a good example of what “system-level” measurement aims for: connecting anonymized exposure to de-identified claims-based outcome reporting, focused on measurement rather than sensitive targeting.
A simple case example (how the system behaves)
Imagine a category launch where:
Linear creates fast national awareness.
CTV extends reach to lighter-linear households and enables sequencing.
Addressable manages household frequency and rotates education vs support messaging.
Search and site content capture intent created by exposure.
A clean-room measurement approach evaluates script lift and regional differences.
Even without perfect attribution, you now have a system where:
TV creates and reinforces memory,
digital captures and educates,
and outcomes measurement is designed for pharma realities.
⚡ When TV is the backbone, digital stops carrying the whole weight.
Rebuilding pharma omnichannel around TV
A rebuild doesn’t start with an upfront plan. It starts with operating principles, then media architecture, then measurement design.
Step 1: Define the backbone role TV will play
Pick one primary job for TV per major initiative:
Category education (condition-first framing)
Brand differentiation (why this option, why now)
Confidence and persistence (support, expectations, adherence cues)
The mistake is trying to do all three at once in every spot.
Step 2: Build a video architecture, not a channel plan
A practical architecture usually includes:
Linear for fast scale and shared context
CTV for incremental reach + sequencing
Addressable for frequency control + message rotation
iSpot’s 2024 data makes the case that the industry is already moving toward cross-platform strategies as streaming momentum grows.
Step 3: Design the “handoff layer” into digital
If TV is the backbone, digital becomes the handoff:
Search strategy aligned to TV claims and condition language
Landing experiences that match the TV promise
FAQ and support content that reduces anxiety and drop-off
Provider discussion guides (where appropriate and compliant)
This is where most omnichannel breaks today: TV says one thing, digital assumes a different intent state.
Step 4: Put frequency and wear-out controls in the plan
Because a huge share of viewing is ad-supported (as mentioned previously), your plan can drift into over-frequency quietly. Use addressable and CTV to manage:
exposure caps at household level (where available),
creative rotation by stage,
and pacing rules that prevent “same spot, same message” fatigue.
Step 5: Build an outcome measurement stack that leadership will trust
And remember: IAB’s 2024 findings suggest the data environment will not get simpler. Build for constraint.
Step 6: Operationalize governance (this is the unglamorous part)
A TV-led omnichannel model tends to fail when:
brand and performance teams optimize against different KPIs,
agencies report in incompatible formats,
and measurement is treated like a post-campaign add-on
Governance fixes that:
one KPI hierarchy,
one definition of “success,”
one cadence for creative and measurement decisions.
With the operating model clear, the natural next question is how teams actually run this without drowning in dashboards and inconsistent reporting.
How AI Digital helps pharma make TV omnichannel-ready
A TV-led omnichannel model adds moving parts fast. The risk is building an analytics project instead of an operating system that helps teams make decisions.
AI Digital is built for that reality. The model is DSP-agnostic, designed to reduce “walled garden” blind spots, and structured around transparent execution and outcome-led optimization.
Here are a few practical ways AI Digital helps pharma make TV omnichannel-ready.
Cross-platform strategy through Open Garden
Major platforms restrict cross-channel visibility, which makes TV + digital coordination harder than it should be. AI Digital’s Open Garden framework is positioned as a neutral alternative, built to unify performance insights across channels instead of keeping them siloed.
Complete transparency into where budget is going (no “black box” buying)
DSP-agnostic execution (AI Digital connects advertisers to 15+ DSPs)
Cross-platform data and insights to improve multi-channel visibility
Managed service execution that includes CTV/OTT
Running TV-led omnichannel means you need consistent planning and optimization across channels, not separate playbooks. AI Digital’s managed service covers end-to-end execution and explicitly includes CTV and OTT within a broader cross-channel mix.
Supply quality and compliance controls with Smart Supply
TV-led omnichannel lives or dies on inventory quality, especially in regulated categories where brand safety and transparency matter. Smart Supply is AI Digital’s programmatic ad buying platform focused on:
filtering low-value or fraudulent traffic before it hits client campaigns
supply path optimization (SPO) to reduce unnecessary ad tech fees
brand safety and compliance with transparent reporting
Elevate for decision support, not just reporting
Elevate is AI Digital’s intelligence platform that combines AI recommendations with human oversight, with a focus on cross-platform insight.
For pharma teams building TV-led omnichannel, the most relevant parts are:
Real-time optimization cadence (campaign parameters adjusted every ~15 minutes)
Predictive planning and automated budget allocation to support KPI-led media decisions
Impact Score System that prioritizes high-impact optimizations
“Ask Elevate” for fast, plain-language interrogation of performance drivers
Multi-touch attribution analysis to understand conversion drivers across touchpoints
All of this supports the broader point of the article: TV becomes more powerful in pharma when it’s planned as part of a measurable system, not treated as a standalone line item.
Conclusion on pharma TV marketing
Pharma marketing doesn’t need another channel trend. It needs a backbone.
TV—linear for scale, CTV for modern delivery, and addressable for control—can provide that backbone because it creates shared context across the journey and supports privacy-safe measurement approaches that align with pharma outcomes. Meanwhile, digital can do what it does best: capture and educate intent, and support the handoffs that TV initiates.
In 2026, the winners won’t be the teams that buy the most CTV. They’ll be the teams that build the cleanest system: one narrative, one architecture, one measurement stack, one governance model.
Blind spot
Key issues
Business impact
AI Digital solution
Lack of transparency in AI models
• Platforms own AI models and train on proprietary data • Brands have little visibility into decision-making • "Walled gardens" restrict data access
• Inefficient ad spend • Limited strategic control • Eroded consumer trust • Potential budget mismanagement
Open Garden framework providing: • Complete transparency • DSP-agnostic execution • Cross-platform data & insights
Optimizing ads vs. optimizing impact
• AI excels at short-term metrics but may struggle with brand building • Consumers can detect AI-generated content • Efficiency might come at cost of authenticity
• Short-term gains at expense of brand health • Potential loss of authentic connection • Reduced effectiveness in storytelling
Smart Supply offering: • Human oversight of AI recommendations • Custom KPI alignment beyond clicks • Brand-safe inventory verification
The illusion of personalization
• Segment optimization rebranded as personalization • First-party data infrastructure challenges • Personalization vs. surveillance concerns
• Potential mismatch between promise and reality • Privacy concerns affecting consumer trust • Cost barriers for smaller businesses
Elevate platform features: • Real-time AI + human intelligence • First-party data activation • Ethical personalization strategies
AI-Driven efficiency vs. decision-making
• AI shifting from tool to decision-maker • Black box optimization like Google Performance Max • Human oversight limitations
• Strategic control loss • Difficulty questioning AI outputs • Inability to measure granular impact • Potential brand damage from mistakes
Managed Service with: • Human strategists overseeing AI • Custom KPI optimization • Complete campaign transparency
Fig. 1. Summary of AI blind spots in advertising
Dimension
Walled garden advantage
Walled garden limitation
Strategic impact
Audience access
Massive, engaged user bases
Limited visibility beyond platform
Reach without understanding
Data control
Sophisticated targeting tools
Data remains siloed within platform
Fragmented customer view
Measurement
Detailed in-platform metrics
Inconsistent cross-platform standards
Difficult performance comparison
Intelligence
Platform-specific insights
Limited data portability
Restricted strategic learning
Optimization
Powerful automated tools
Black-box algorithms
Reduced marketer control
Fig. 2. Strategic trade-offs in walled garden advertising.
Core issue
Platform priority
Walled garden limitation
Real-world example
Attribution opacity
Claiming maximum credit for conversions
Limited visibility into true conversion paths
Meta and TikTok's conflicting attribution models after iOS privacy updates
Data restrictions
Maintaining proprietary data control
Inability to combine platform data with other sources
Amazon DSP's limitations on detailed performance data exports
Cross-channel blindspots
Keeping advertisers within ecosystem
Fragmented view of customer journey
YouTube/DV360 campaigns lacking integration with non-Google platforms
Black box algorithms
Optimizing for platform revenue
Reduced control over campaign execution
Self-serve platforms using opaque ML models with little advertiser input
Performance reporting
Presenting platform in best light
Discrepancies between platform-reported and independently measured results
Consistently higher performance metrics in platform reports vs. third-party measurement
Fig. 1. The Walled garden misalignment: Platform interests vs. advertiser needs.
Key dimension
Challenge
Strategic imperative
ROAS volatility
Softer returns across digital channels
Shift from soft KPIs to measurable revenue impact
Media planning
Static plans no longer effective
Develop agile, modular approaches adaptable to changing conditions
Brand/performance
Traditional division dissolving
Create full-funnel strategies balancing long-term equity with short-term conversion
Capability
Key features
Benefits
Performance data
Elevate forecasting tool
• Vertical-specific insights • Historical data from past economic turbulence • "Cascade planning" functionality • Real-time adaptation
• Provides agility to adjust campaign strategy based on performance • Shows which media channels work best to drive efficient and effective performance • Confident budget reallocation • Reduces reaction time to market shifts
• Dataset from 10,000+ campaigns • Cuts response time from weeks to minutes
• Reaches people most likely to buy • Avoids wasted impressions and budgets on poor-performing placements • Context-aligned messaging
• 25+ billion bid requests analyzed daily • 18% improvement in working media efficiency • 26% increase in engagement during recessions
Full-funnel accountability
• Links awareness campaigns to lower funnel outcomes • Tests if ads actually drive new business • Measures brand perception changes • "Ask Elevate" AI Chat Assistant
• Upper-funnel to outcome connection • Sentiment shift tracking • Personalized messaging • Helps balance immediate sales vs. long-term brand building
• Natural language data queries • True business impact measurement
Open Garden approach
• Cross-platform and channel planning • Not locked into specific platforms • Unified cross-platform reach • Shows exactly where money is spent
• Reduces complexity across channels • Performance-based ad placement • Rapid budget reallocation • Eliminates platform-specific commitments and provides platform-based optimization and agility
• Coverage across all inventory sources • Provides full visibility into spending • Avoids the inability to pivot across platform as you’re not in a singular platform
Fig. 1. How AI Digital helps during economic uncertainty.
Trend
What it means for marketers
Supply & demand lines are blurring
Platforms from Google (P-Max) to Microsoft are merging optimization and inventory in one opaque box. Expect more bundled “best available” media where the algorithm, not the trader, decides channel and publisher mix.
Walled gardens get taller
Microsoft’s O&O set now spans Bing, Xbox, Outlook, Edge and LinkedIn, which just launched revenue-sharing video programs to lure creators and ad dollars. (Business Insider)
Retail & commerce media shape strategy
Microsoft’s Curate lets retailers and data owners package first-party segments, an echo of Amazon’s and Walmart’s approaches. Agencies must master seller-defined audiences as well as buyer-side tactics.
AI oversight becomes critical
Closed AI bidding means fewer levers for traders. Independent verification, incrementality testing and commercial guardrails rise in importance.
Fig. 1. Platform trends and their implications.
Metric
Connected TV (CTV)
Linear TV
Video Completion Rate
94.5%
70%
Purchase Rate After Ad
23%
12%
Ad Attention Rate
57% (prefer CTV ads)
54.5%
Viewer Reach (U.S.)
85% of households
228 million viewers
Retail Media Trends 2025
Access Complete consumer behaviour analyses and competitor benchmarks.
Identify and categorize audience groups based on behaviors, preferences, and characteristics
Michaels Stores: Implemented a genAI platform that increased email personalization from 20% to 95%, leading to a 41% boost in SMS click through rates and a 25% increase in engagement.
Estée Lauder: Partnered with Google Cloud to leverage genAI technologies for real-time consumer feedback monitoring and analyzing consumer sentiment across various channels.
High
Medium
Automated ad campaigns
Automate ad creation, placement, and optimization across various platforms
Showmax: Partnered with AI firms toautomate ad creation and testing, reducing production time by 70% while streamlining their quality assurance process.
Headway: Employed AI tools for ad creation and optimization, boosting performance by 40% and reaching 3.3 billion impressions while incorporating AI-generated content in 20% of their paid campaigns.
High
High
Brand sentiment tracking
Monitor and analyze public opinion about a brand across multiple channels in real time
L’Oréal: Analyzed millions of online comments, images, and videos to identify potential product innovation opportunities, effectively tracking brand sentiment and consumer trends.
Kellogg Company: Used AI to scan trending recipes featuring cereal, leveraging this data to launch targeted social campaigns that capitalize on positive brand sentiment and culinary trends.
High
Low
Campaign strategy optimization
Analyze data to predict optimal campaign approaches, channels, and timing
DoorDash: Leveraged Google’s AI-powered Demand Gen tool, which boosted its conversion rate by 15 times and improved cost per action efficiency by 50% compared with previous campaigns.
Kitsch: Employed Meta’s Advantage+ shopping campaigns with AI-powered tools to optimize campaigns, identifying and delivering top-performing ads to high-value consumers.
High
High
Content strategy
Generate content ideas, predict performance, and optimize distribution strategies
JPMorgan Chase: Collaborated with Persado to develop LLMs for marketing copy, achieving up to 450% higher clickthrough rates compared with human-written ads in pilot tests.
Hotel Chocolat: Employed genAI for concept development and production of its Velvetiser TV ad, which earned the highest-ever System1 score for adomestic appliance commercial.
High
High
Personalization strategy development
Create tailored messaging and experiences for consumers at scale
Stitch Fix: Uses genAI to help stylists interpret customer feedback and provide product recommendations, effectively personalizing shopping experiences.
Instacart: Uses genAI to offer customers personalized recipes, mealplanning ideas, and shopping lists based on individual preferences and habits.
Medium
Medium
Share article
Url copied to clipboard
No items found.
Subscribe to our Newsletter
THANK YOU FOR YOUR SUBSCRIPTION
Oops! Something went wrong while submitting the form.
Questions? We have answers
How do TV and digital channels work together effectively?
TV creates broad, shared awareness and makes the message memorable, while digital captures and deepens intent—search, landing pages, and HCP/patient resources handle the next steps. The key is consistency: align the TV claim language with what people will search, send them to a page that matches the promise, and use CTV or retargeting to reinforce the message without overserving the same creative.
What are the most effective TV formats for pharma campaigns?
Linear TV is strongest for fast scale and mass education, especially for launches and category framing. CTV is effective for incremental reach and sequencing messages to different audience segments over time. Addressable TV is most useful for frequency control and rotating creative variations by non-sensitive proxies like geography or life stage, which helps reduce fatigue and improve efficiency.
How can AI improve omnichannel engagement?
AI helps by turning fragmented signals into actionable decisions—choosing the next best message, pacing spend across channels, and spotting where the journey is breaking (for example, strong reach but weak follow-through). It’s most valuable when it supports governance, forecasting, and continuous optimization rather than simply producing more dashboards.
What is the easiest way to combine TV and digital campaigns?
Start with one shared audience definition and one core narrative, then build a simple handoff: TV drives to search and a dedicated landing experience, digital reinforces the same message and answers the “what now?” questions, and measurement ties exposure to agreed outcomes using a small set of KPIs. If you only do one thing, make sure the TV message and the landing page feel like the same conversation.
What is pharma TV marketing, and why does it still matter?
Pharma TV marketing is the use of linear TV, CTV, and addressable TV to build awareness, educate patients and caregivers, and reinforce brand confidence at scale. It still matters because pharmaceutical advertising often needs shared, trusted context before people search, ask a doctor, or take the next step.
How does TV in pharma marketing support HCP engagement without replacing professional channels?
TV in pharma marketing can prime patient conversations, which often changes the quality of HCP engagement in the exam room, even if the media wasn’t targeted to clinicians. When paired with aligned HCP resources and field materials, TV helps create continuity between what patients ask and what providers can confidently discuss.
What’s the biggest mistake pharma brands make in pharmaceutical advertising across TV and digital?
The most common mistake is treating TV as “awareness only” and digital as “performance,” then measuring them with incompatible KPIs. Pharmaceutical advertising works better when TV creates demand and memory while digital captures and educates that demand, using one shared outcome hierarchy.
Have other questions?
If you have more questions, contact us so we can help.
Questions? We have answers
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.
This is some text inside of a div block.
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Suspendisse varius enim in eros elementum tristique. Duis cursus, mi quis viverra ornare, eros dolor interdum nulla, ut commodo diam libero vitae erat. Aenean faucibus nibh et justo cursus id rutrum lorem imperdiet. Nunc ut sem vitae risus tristique posuere.


.svg)
.svg)